Breast augmentation is a very commonly performed cosmetic surgical procedure. In 1998, survey figures reveal that 34% of North American women are dissatisfied with their breasts. In 2003, breast augmentation was the third most common cosmetic surgical procedure performed by members of the American Society of Plastic Surgery (with only Botox injections and microdermabrasion being more common).
Breast augmentation is designed to add volume and improve the shape of a small breast or restore breast volume lost through childbirth, weight loss or age. This is done by the insertion of a breast implant. In addition, or alternatively, your plastic surgeon may recommend a breast lift to restore a more youthful shape and nipple-areolar position to the breast.
Insertion of a breast implant will hide a small amount of breast tissue from mammogram assessments. Each patient needs to discuss breast cancer detection with their surgeon and should strongly consider their choice for breast augmentation if a family history of breast cancer exists.

IDEAL CANDIDATE
Younger woman with a normal breast examination, no personal or family history of breast cancer, small breast size and without inherent breast abnormalities.
LOCATION
Breast augmentation (‘augmentation mammoplasty’) is performed as an outpatient procedure under general or a combination of local and regional anesthesia, in a hospital or surgical clinic setting. You should be accompanied home from your surgery and have someone with you on the night after your surgery.
CONTRAINDICATIONS (some may be relative)
- Multiple surgical procedures on the breasts
- Undiagnosed breast lump(s) or known breast cancer
- Obesity
- Likely or planned future pregnancy
- Medical conditions prohibiting elective surgery
- Unrealistic expectations
PREPARATION
Prior to any plastic surgical procedure patients should avoid alcoholic beverages for one week prior to surgery. Anti-inflammatory drugs (Aspirin®, Motrin®, Ibuprophen, Advil®, etc.) should stopped two weeks prior to surgery due to their effects on the body’s blood clotting system. Failure to do so may lead to increased bleeding during the operation, blood clots (hematomas) and post-operative bruising. If you require painkillers on a regular basis for arthritic pain or headaches, the use of Tylenol ES® will not affect blood clotting. The use of herbal supplements or traditional medicines should be discussed with your surgeon pre-operatively to see if they will affect your surgery.
All medical conditions and medications must be disclosed to your surgeon pre-operatively. Medical conditions such as high blood pressure must be well controlled before all cosmetic procedures where bleeding and hematomas are a risk.
Smoking requires special mention as chemicals in smoke can cause vasoconstriction of blood vessels resulting in reduced blood supply to the redraped body tissue. Smoking should be stopped 2-3 months before the operation in order to eliminate the added risk of tissue loss due to smoking. Some surgeons will refuse to perform elective cosmetic operations on smokers due to this risk.
A variety of choices must be entertained before selecting the ideal procedure for any candidate. First, the size of augmentation (implant) desired; second, the type of implant (saline or silicone; round or anatomic; textured or non-textured); third, the proposed location for the implant (behind the breast but in front of the chest muscles, partially behind the chest muscles, totally behind the chest muscles); and fourth, the surgical approach to that location (pocket). As many of these choices must be made on an individual basis, an in depth discussion with your surgeon will highlight many of the pros and cons of these various choices and help you with your decision.
THE IMPLANTS
Breast implants have undergone many revisions since their original introduction to the commercial marketplace in the early 1960’s. Failures of some of the second generation silicone implants and public concern over possible adverse health effects of the silicone lead to the moratorium on silicone implants imposed in 1992. Since that time, there have been extensive studies to address the proposed connection between silicone and the adverse heath problems that
Today, fourth-generation breast implants are made of a silicone shell filled with sterile salt water (saline implant), or weakly cross-linked silicone gel (standard silicone implant). Most recently, cohesive gel (form stable silicone implant) implants have been introduced on the market with the added safety profile of lessened gel bleed. The silicone implants of today are fourth generation implants and do not carry the same degree of risk as those of yesteryear.
Implants come in various sizes and profiles. Your plastic surgeon will help you select an appropriate implant size and profile for your body frame based on your anatomy and your desires.
Both cohesive and non-cohesive silicone gel implants are now available for breast augmentation in Canada. Currently, saline implants remain the most popular implant of choice but this may change with reintroduction of silicone implants to the cosmetic marketplace.
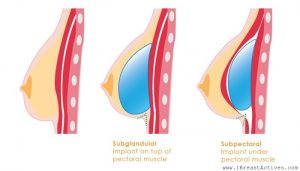
IMPLANT PLACEMENT
Breast implants are placed into tissue pockets created below the glandular breast (subglandular), below the chest wall muscles (submuscular).
|
Subglandular Implants |
|
|
Advantages |
Disadvantages |
|
|
|
Submuscular Implants |
|
|
Advantages |
Disadvantages |
|
|
Discuss implant location with your plastic surgeon and have a clear understanding of all benefits and disadvantages before making the choice that is right for you.
THE PROCEDURE
An incision is made at the edge of the areola (periareolar), under the breast (inframammary), or in the armpit (axillary). Difficulties in breast-feeding have been reported with some approaches.
Dissection is performed to create a pocket for implant placement under the glandular breast itself (subglandular location) or under the muscles of the chest wall (submuscular location). A pocket combining both planes (dual-plane) may also be employed. The implant is inserted and filling is performed if a saline implant is used. Incisions are closed and dressings are placed. Many surgeons employ elastic dressings or special tapes to assist in maintaining implant location in the early post-operative period.
The TUBA (Trans-Umbilical Breast Augmentation) technique was designed as an endoscopic means to insert breast implants through the belly button and avoid scars on the breast itself. It is a procedure not offered by many surgeons and considered by most as an inferior option due to its high-technical nature and great distance from between the incision and operative site. Most surgeons believe that this complexity sacrifices control of the implantation process to avoid scars that are very good to excellent in the hands of most plastic surgeons.
THE RECOVERY
The typical convalescence following breast augmentation is 3-4 weeks. A contouring garment or bra is often used in the early post-operative period. Pain is controlled with prescription medications for the first days to week. Most patients require only over-the-counter medications or are comfortable without pain medication within days of the procedure. Stool softeners may be helpful if prolonged use of prescription narcotic medication is required. Bruising and swelling of can become more noticeable after 3-4 days. Remember that this is a normal part of recovery and disappears within 2-3 weeks of the procedure. If your surgeons recommends you wear a bra without an under wire, you can simply make a small cut in the fabric and slide out the wire. This can be replaced and re-stitched at a later date.
Remember, it is a good idea to take some time off work. I usually recommend a week with the option to take additional time if required. To make things easier on yourself clean house and do chores that are more physical prior to your surgery as you won’t feel like doing them for at least a week. Having some prepared meals and lowering items on shelves may be helpful so you don’t have to do too much overhead reaching in the first couple of weeks. Arranging assistance for childcare in the first few days will be a big help.
Work activities should be avoided for 2-4 weeks and longer in cases of manual labor. Allow 3-4 days before engaging in any activities that require much arm use. Activities that cause a natural rise in blood pressure should be avoided for 2 weeks (yes this includes sex). Sports may be resumed after 1-2 months. Everyone recovers differently so listen to your body.
POTENTIAL COMPLICATIONS
Any form of surgery carries risks. Although these risks are uncommon, it is important that they are discussed between the patient and surgeon. Some potential risks are listed in the table below.
|
Intra-operative |
Early Post-operative |
Late Post-operative |
|
|
|
*Formation of a fibrous capsule around ANY foreign body is a normal part of your body’s healing. Excessive formation resulting in deformity of the implant is termed a capsular contracture.
† Complication rates rise with larger implants in all cases
For a more detailed discussion on expected results, recovery, and specific complications, please see your individual surgeon.
WHAT TO EXPECT
In spite of individual differences in pain perception, post-operative pain is often underestimated, especially following submuscular implantation. Recently, new techniques have arisen to help deal with this problem. Another note is that implants may sit very high (on the chest wall) in the early post-operative period and are expected to settle some (over the next 4-8 weeks). Women comment on the initial firmness of the breast that appears to soften with time but obviously never reach the consistency of normal breast tissue. Bruising in the axillary (arm pit) or abdominal region may be significant with either the trans-axillary or TUBA procedures.
Breast scars will take approximately 12-18 months before they can be assessed in their final form. During that time protection of the scars from the sun is essential. During that time protection of the scars from the sun is essential. Although proper sun protection is essential on all exposed skin, high SPF sunscreens (SPF 45 0r 60) are essential over the surgical scars, for 12-18 months, to prevent permanent darkening of the scars. Often these scars are very good to excellent. Residual breast numbness may occur but is exceedingly rare. If you started out with some breast sag (ptosis) the addition of the volume replaced or added by the implant appears to mostly if not completely reverse this appearance. In addition to the breast lift, the additional volume often fills the skin and “pseudo-blanches” the appearances of stretch marks, making them less noticeable. Remember that it is possible to get new stretch marks secondary to the augmentation process if you request very large augments for your body size. These usually lighten with time but never disappear. In general, patient satisfaction with this procedure is extremely high.
COST
Breast augmentation surgery is not covered under the Canadian Medical Plan and the final cost for such procedures will be at the discretion of the plastic surgeon performing the procedure. The average cost of this procedure, published by the Canadian Society of Aesthetic (Cosmetic) Plastic Surgery (CASPS) is $6000 (with a range of $6000-$12,000). Costs will vary based on the implant type used.
DISCLAIMER
This website does not cover all of the medical knowledge related to breast augmentation nor does it deal with all possible risks and complications of surgery on the breasts. Although it is designed to provide the patient with greater depth of information in some areas, it is not intended to substitute for the in depth discussion between patient and surgeon that must occur prior to any surgical procedure.